A Supraventricular Tachycardia (SVT) is one that originates above the ventricles. The same irritable foci discussed in tutorial 5 may fire repeatedly with a rapid rate. If this happens, the SA node will never get a chance to fire and we call the rhythm a tachycardia if the rate > 100. An SVT may alternatively be caused by a reentrant loop as in Wolff-Parkinson-White syndrome or if the rhythm is irregular, by a fast ventricular response to atrial fibrillation.
SVT usually have a narrow QRS since the waves of depolarization are conducted through the AV node down the bundle branches into the ventricles. However, our lesson from the previous tutorial applies here:
Importantly, note that a narrow QRS tachycardia must originate above the ventricles. It may come from the atria or the AV node, but not from the ventricles.
We will not discuss all possible SVTs here, but only a few representative ones.
Sinus tachycardia refers to a tachycardia generated by the SA node - i.e. the heart is beating fast because the SA node pacemaker is telling it to beat fast. The patient was running or the patient has a fever, or the patient has had too much coffee, or the patient was injected with epinephrine, or the patient has hyperthyroidism - many things can cause sinus tachycardia.
An upper limit on the rate of a sinus tachycardia can be given in terms of the patient's age:
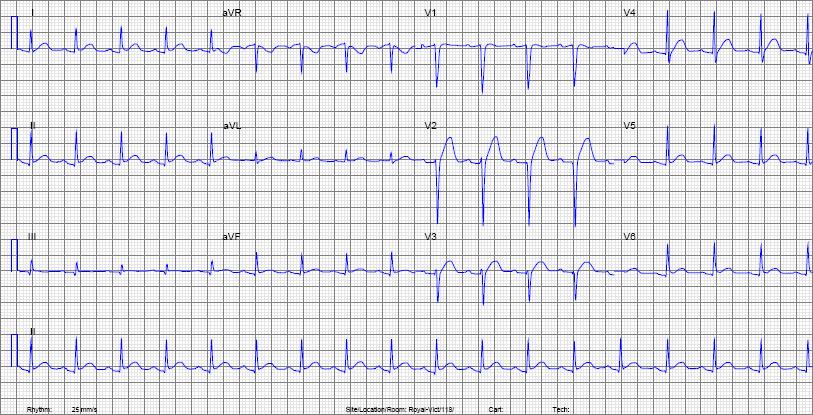
| Rate | around 108 |
| Rhythm | Regular sinus rhythm - there is a P wave before each QRS and the P waves are up in II and down in aVR. |
An ectopic atrial tachycardia is one that is produced by an irritable atrial focus. The rate may exceed the speed limit of 220-age and the P-waves may have an abnormal morphology since they originate outside the SA node.
PSVTs are tachycardias that arise instantly, the patient may feel their heart rate jump suddenly from 60 to 220. Paroxysmal means of sudden onset - one gets an "attack" of PSVT, one does not get an attack of sinus tachycardia. Sinus tachycardia comes on gradually.
One may not be able to differentiate a PSVT from an sinus tachycardia on an EKG unless the P-waves are abnormal or we catch beginning of the arrhythmia on the EKG (e.g. with a Holter). The distinction may have to be made clinically and confirmed by Holter or another method.
Possible causes of PSVT include:
As mentioned above, it may not be possible when reading an ECG to tell the difference between a PSVT or another form of SVT. If the rhythm is fast enough that P-waves would not be distinguishable, but slower than the speed limit of 220-age, then we might have to consider sinus tachycardia also.
Now analyse the rate and rhythm of the following EKG obtained from a 48 year old woman:
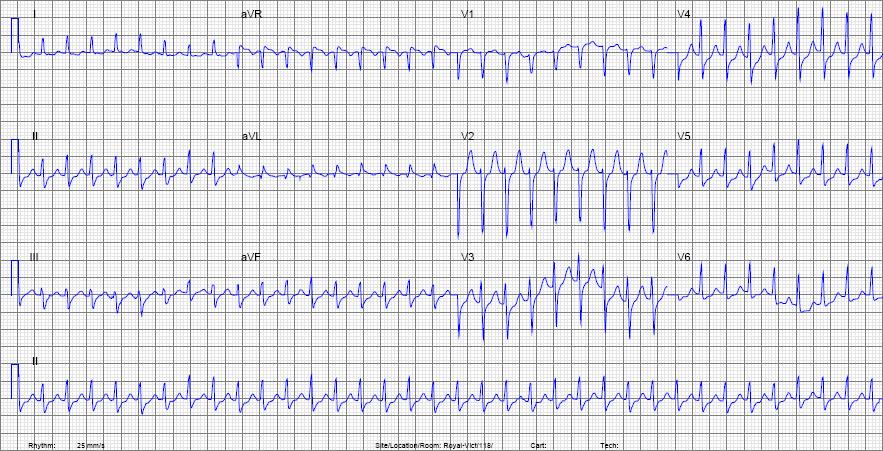
| Rate | around 210 which is faster than the speed limit of 174 - therefore this is NOT a sinus tachycardia. |
| Rhythm | Regular with a narrow QRS. The P-waves (if there are any) are buried in the T-waves and we can't comment on their morphology. Since we are not given any history and have no further information, we can comment only that the rhythm is an SVT and definitely not a sinus tachycardia. |