|
Blood
Laboratory |
Erythrocyte sedimentation rate (ESR) |
| |
The ESR is a simple non-specific screening
test that indirectly measures the presence of inflammation in the body.
It reflects the tendency of red blood cells to settle more rapidly in
the face of some disease states, usually because of increases in plasma
fibrinogen, immunoglobulins, and other acute-phase reaction proteins.
Changes in red cell shape or numbers may also affect the ESR. |
|
Method |
|
|
When anticoagulated whole blood is allowed
to stand in a narrow vertical tube for a period of time, the RBCs –
under the influence of gravity - settle out from the plasma. The rate at
which they settle is measured as the number of millimeters of clear
plasma present at the top of the column after one hour (mm/hr). |
|

The Wintrobe
sedimentation rack
There are two main methods used to measure the ESR: the Westergren method and
the Wintrobe Method. Each method produces slightly different results.
Most laboratories use the Westergren method. |
Westergren method:
The Westergren method requires collecting 2 ml of venous
blood into a tube containing 0 .5 ml of sodium citrate. It should be stored no longer than 2 hours at room temperature
or 6 hours at 4 °C. The blood is drawn into a Westergren-Katz tube to the 200 mm mark. The tube is placed
in a rack in a strictly vertical position for 1 hour at room
temperature, at which time the distance from the lowest
point of the surface meniscus to the upper limit of the red
cell sediment is measured. The distance of fall of erythrocytes,
expressed as millimeters in 1 hour, is the ESR.
|
 |
Wintrobe method:
The Wintrobe method is performed similarly except that the Wintrobe
tube is smaller in diameter than the Westergren tube and only 100 mm
long. EDTA anticoagulated blood without extra diluent is drawn into the
tube, and the rate of fall of red blood cells is measured in millimeters
after 1 hour. The shorter column makes this method less sensitive
than the Westergren method because the maximal possible abnormal value
is lower. However, this method is more practical for demonstration
purposes.
|
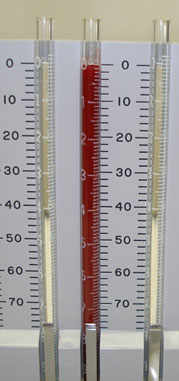
This picture shows a rack holding Wintrobe
tubes, in which anticoagulated whole blood has just been added.
(Time: 0) |
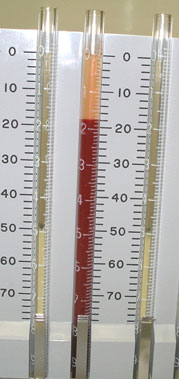
Red blood cells have settled, leaving plasma
at the top of the tube. Reading: 18 mm/hour
(Time: one hour)
|
|
Average values in healthy men are: <15mm/hr;
in healthy females, they are somewhat higher: <20mm. The values are
slightly higher in old age, in both genders. |
|
Theoretical considerations
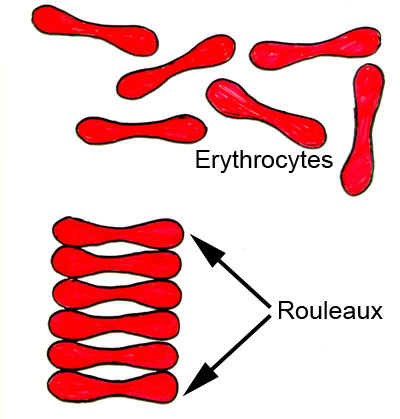
The RBCs sediment because their density is
greater than that of plasma; this is particularly so, when there is an
alteration in the distribution of charges on the surface of the RBC
(which normally keeps them separate form each other) resulting in their
coming together to form large aggregates known as rouleaux. |
 |
|
Rouleaux formation is
determined largely by increased levels of plasma fibrinogen and
globulins, and so the ESR reflects mainly changes in the plasma proteins
that accompany acute and chronic infections, some tumors and
degenerative diseases. In such situations, the ESR values are much
greater than 20mm/hr. Note that the ESR denotes merely the presence of
tissue damage or disease, but not its severity; it may be used to follow the progress of the
diseased state, or monitor the effectiveness of treatment. |
|
Some interferences which increase ESR: |
-
increased level of
fibrinogen, gamma globulins.
-
technical factors:
tilted ESR tube, high room temperature.
|
|
Some interferences which decrease ESR: |
- abnormally shaped RBC (sickle cells,
spherocytosis).
- technical factors: short ESR tubes,
low room temperature, delay in test performance (>2 hours), clotted
blood sample, excess anticoagulant, bubbles in tube.
|
| Chronic inflammatory disease
(collagen and vascular diseases) increases ESR. |
| Polycythemia decreases ESR. |
|
| |
|
Click here to continue with the topic of
hemostasis |